2/2 also stay tuned for "Q & A with Dr. JOSE"- a public education project w/ Dr. Jose Morales dedicated to our family & friends & BIPOC communities b/c we're still in a pandemic! #MaskUp & Learn why getting #vaccinated is the best way to protect yourself & the people you LOVE!
1/2 For folks who seek science, check out this event on @BronxnetTV & also follow Dr. Jose at @josefmo and his blog! @ScienceMagazine is cool but Dr. Jose is my "go to" as far as Puerto Rican biologists go! 🇵🇷 https://t.co/sVIPY0jusZ
The FDA advisory panel will release their recommendations on Booster shots later today. One thing that I have noted in reading press reports is the absence of discussion of whether vaccines should be sent abroad to places where people aren’t getting vaccinations. American’s are not getting the information that sending vaccines abroad will protect American’s.
I can’t help but think that skewed framing arises from fears of the right-wing in this country. Commentators may be fearing that they will be charged with putting the lives of THOSE PEOPLE ahead of American lives. I worry that the increasingly extreme belligerency of the right is silencing the discussion of the how vaccinating the world is the best protection for all people including Americans.
At least in the US, folks know that for the right wing, our lives matter more than their lives. What would be really crazy making is if the right thinks this is the terms of the discussion. They may completely misunderstand what will keep Americans safe. Who knows! Maybe they do understand and just don’t care. I have to say, I won’t be surprised at anything coming from the US right wing nowadays and for the foreseeable future.
Bottom line, we need to send vaccines abroad and the press has to explain why.
Wealth inequality is a critical problem in the US and is especially acute in the global context. Unsurprisingly, during the Covid pandemic, the global wealth inequality has borne “vaccine inequality” or the uneven distribution of Covid vaccines. Most recently, the USA and developed countries have seen the emergence of a “vaccine inequality” flashpoint. Should fully vaccinated US people be given a 3rd shot or “Booster” – OR – should a larger portion of humanity residing in the Developing world be given their 1st shot? In short, Boosters or abroad?
Responding to the idea of boosters, many concerned for the Developing world express consternation. For example… “Instead of solving the problem by vaccinating the world and cutting off new variants, rich countries seem prepared to fork over more money for boosters, and live in a state of endless fear…”US citizens and policy makers must grapple with this consequential decision.
The accompanying articles from major news and science outlets journals explore this issue.
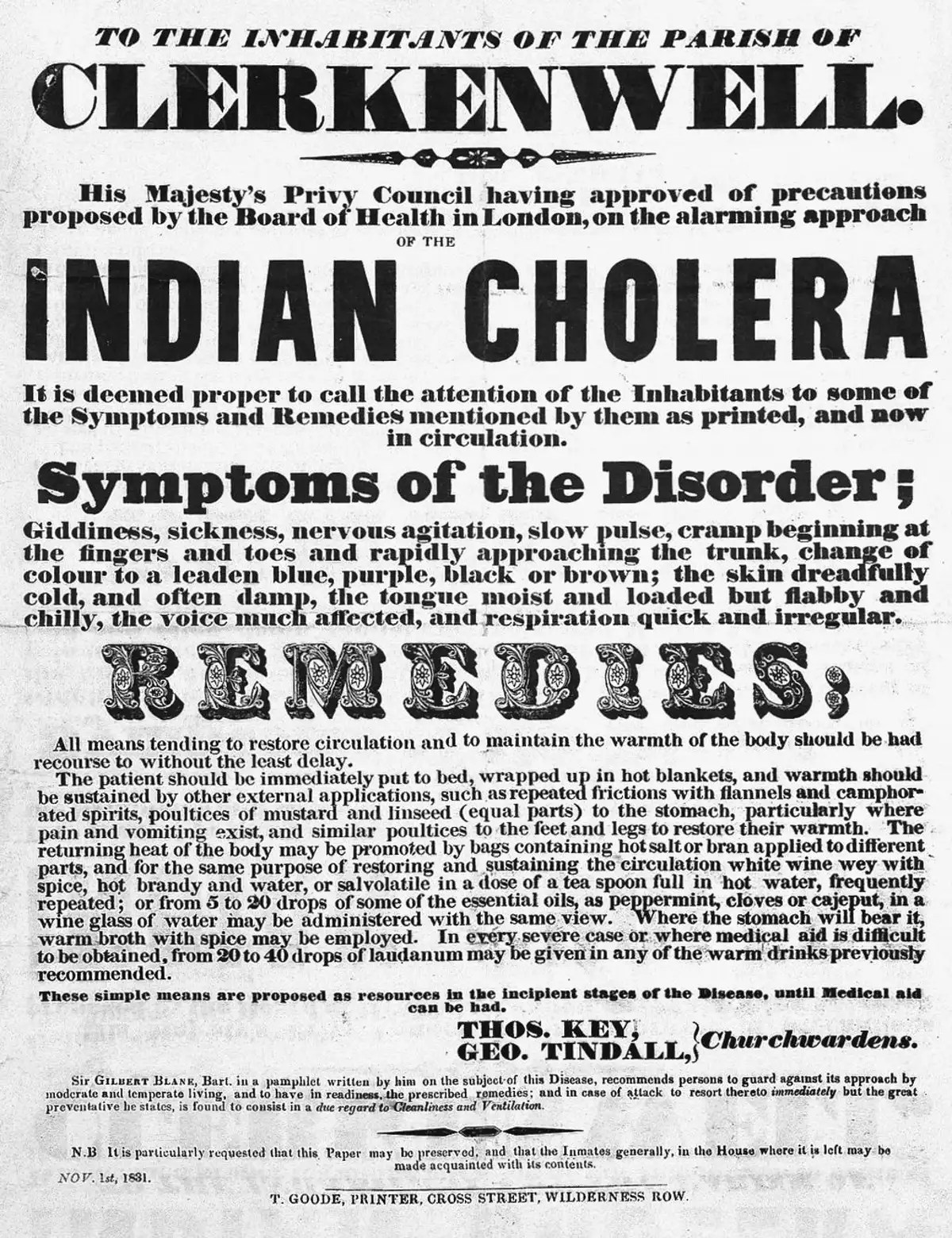
The purpose of this post is to answer this question. I contend that disease history provides tools to guide our steps forward. I propose that, as we approach the 200 anniversary of the UK’s first cholera case in 1831, that cholera’s history may serve as a lens to sharpen our focus on this issue.
In this historical analogy, mid 18th Century London stands in for today’s entire world. As London had its wealthy and poor denizens, so the world has its developed and developing countries. As conditions of life in London at that time are relevant, so are the world’s conditions of life today. As Londoners suffered epidemics of cholera, so does humanity suffer from the Covid pandemic.
Remarkably, the similarities continue. When cholera spread from the Indian subcontinent to Europe, efforts were made to prevent the arrival of the disease with a quarantine of incoming ships. Today, the USA and European countries sought to stop Covid’s spread by limiting air travel to their countries.
European physicians were entirely unfamiliar with cholera’s symptoms, prognosis, transmission, treatments or cure. Analogously, Covid was unknown to science resulting in ignorance of Covid’s disease characteristics, as well as treatments or vaccines. Cholera’s terrifying symptoms and course prodded the English public’s imagination seeing it as a foreign epidemic (‘Asiatic cholera’) ‘invading’ the nation. Today, US politicians saw Covid as a foreign epidemic dubbing it the “Kung Flu” or the “China virus”.
A bitter irony is that while the scourge of cholera is in London’s past, many curable diseases, LIKE cholera, devastate developing countries today. Cholera remains a threat because the WHO estimates that 78% of people in the Developing world lack clean water supplies, and 85% are without adequate sewage infrastructure.
Unclean water supply in Yemen
POVERTY AND DISEASE
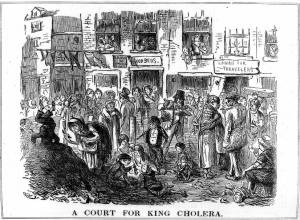
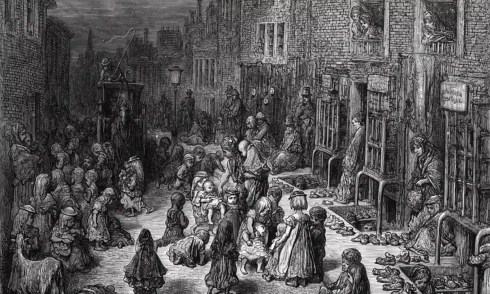
For the Developed world to learn from its own history, we turn to London some 200 hundred years ago. In the midst of a rapid industrialization and urbanization, it was clear that a major facet of life was the growing gulf between rich and poor. The daily life of London’s poor was in the squalor of overcrowded slums. Human waste was heaped in courtyards, and filth from the flooding of basement cesspits swamped into the gutters and waterways in that sewer-less era.
Unfortunately, today, much of the world’s people contend with similar issues of poverty, housing and sanitation. Today’s world has hundreds of millions living in extreme poverty, 1.6 billion people live in inadequate shelter and 55% of the global population do not use a safely managed sanitation service. Today, around 2.2 billion people are without access to safe drinking water and 1 in 9 people world-wide is hungry or undernourished.
CONDITIONS PROVOKE DISEASE
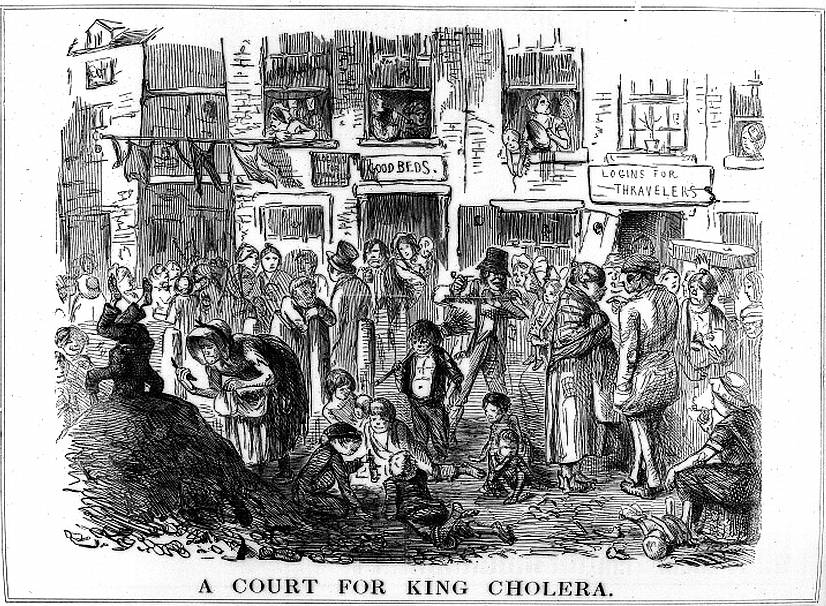
Clearly, cholera was connected to the conditions of life of the city’s poor. From every cholera epidemic for which statistics are available, the malady found an excessive number of its victims from London’s poverty-stricken corners. Cholera appeared confined to the shacks and hovels of the new industrial districts, with the disease’s hardest blow’s falling upon those described as“… the destitute, the intemperate, and the degraded.”
The Londoners confronting cholera soon understood that those conditions ushered in four outbreaks of cholera and thousands of deaths. Indeed, observers noted that “It is in a nation’s dens of poverty … that the cholera is engendered…”
Edwin Chadwick
Various figures played important roles in meeting these challenges. Among them was Edwin Chadwick, a public health campaigner who was tasked with tackling public sanitation. He bucked the dominant view at the time that disease and urban poverty resulted from bad habits and flawed character. Instead, in “The Sanitary Conditions of the Laboring Population (1842)”, Chadwick proposed a direct link between poor living conditions, disease and life expectancy. He urged that rapid population growth, overcrowded housing and sanitation problems needed to be addressed to curb cholera’s spread. New York City, suffering similar epidemics at that same time, prompted an observer to observe that cholera was “a scourge of our vicious social state.”
Unsurprisingly, just as conditions of life in London slums made cholera possible, so does the Developing world’s current conditions also set the stage for the Covid pandemic. The developing nations confront Covid with meager health systems incapable of basic services, fragile economic systems and severely restricted financial resources. Further, they meet the pandemic with scant skilled services and a poorly educated populace. For instance, there is only 1 doctor for over 2000 inhabitants in Sub-Saharan African and South East Asian countries. Necessarily, Covid’s impact on the Developing world will be much more severe with devastating social and economic consequences.
EVERYONE IS AFFECTED
London’s detestable living conditions and cholera spread were not confined to the slums of the poor. For example, Parliament was prompted to close for a time because of the raw sewage stench of the River Thames and the accompanying fear of smell’s ability to provoke disease . Many observers at the time registered cholera’s indifference to wealth or status as the comments clearly show.
“The pestilence was literally sweeping everything before it, neither age, nor sex, nor station escaping.”
“During this outbreak …There was apparently no discrimination between the houses of the rich and those of the poor.
“Not the poor and the vicious classes alone will fall victims to the coming pestilence… will infect and kill many persons among the more favored class.”
John Snow
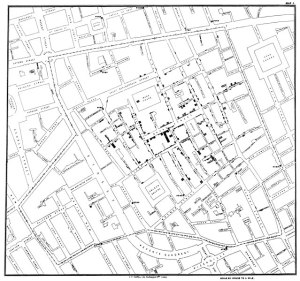
When those of higher station recognized cholera’s disdain for boundaries of wealth in the fourth outbreak, ingenuity was fully brought to bear on the crisis. In 1854, Soho, a suburb of London, felt the ravages of a terrible cholera outbreak. Soho was, at the time, the most densely populated district in greater London. Soho was an economically diverse neighborhood with a wide array of businesses, residences and industry. The people were a mix of destitute, poor, working poor and merchants, nestled amidst the more opulent quarters of the favored classes. The physician John Snow, now known as the pioneer of public health research in a field known as epidemiology, lived near Soho. This proximity likely influenced Snow’s considerable efforts to evaluate his theory that contaminated water was the cause of the outbreak.
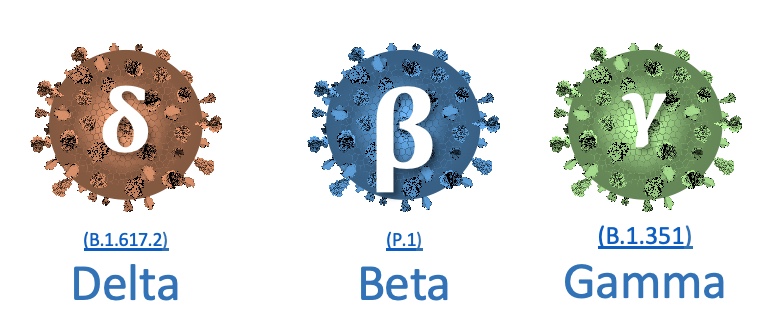
Today, Covid mirrors cholera’s disregard of affluence spreading to all countries and classes. Indeed, when spread seemed imminent upon crossing international borders, Covid grabbed the full attention of the Developed world. For example, a month after the WHO declared Covid a global emergency, did US citizens became infected and the government put forward pandemic response plans. Additional measures were invoked when (D, B, G) variants from the Developing world displayed even greater enthusiasm for homo sapiens of every class and station.
CITY STRUCTURAL CHANGES
London’s upper classes, after the illness and death of thousands of its poor, ultimately grasped that only with London-wide, large-scale action would cholera finally yield. Thus, the decision makers undertook city-wide structural changes that affected all of London’s peoples.
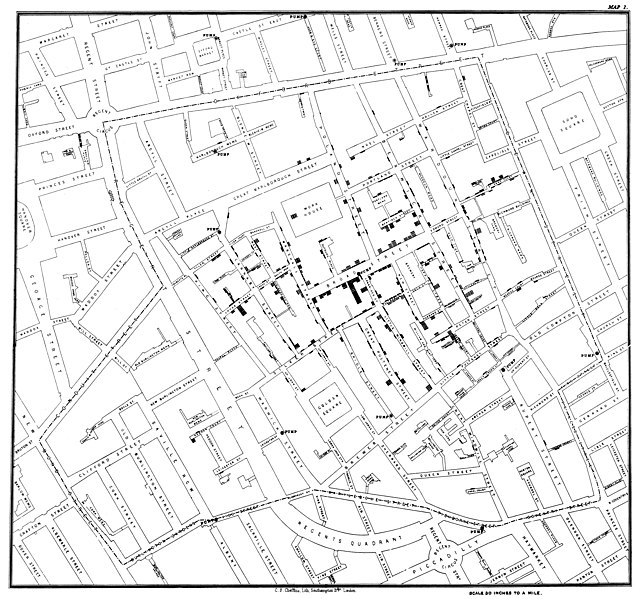
Original map made by John Snow in 1854. Cholera cases are highlighted in black.
Starting from the foundation of understanding the problem, doctors and reformers like as Edwin Chadwick, William Farr, and John-Simon had helped communicate the dangers of poor drainage, foul water, and crowded tenements. They advanced the notion that disease had to be prevented through cleanliness and sanitation. Later, the Reverend Henry Whitehead and physician John Snow, used rigorous empiricism, statistics and disease maps to prove the theory that the cholera outbreak cause was contaminated water.
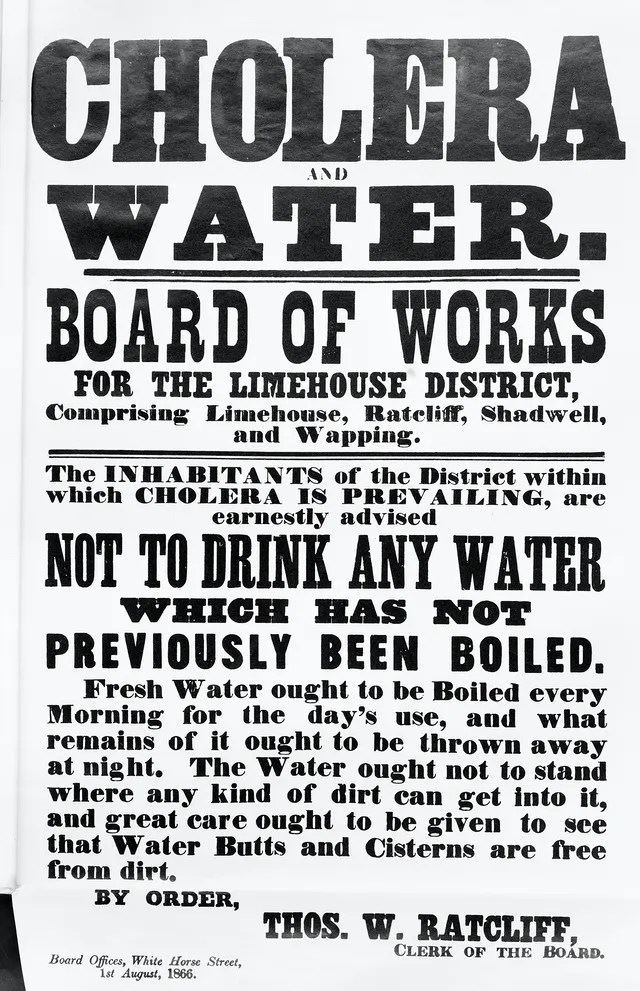
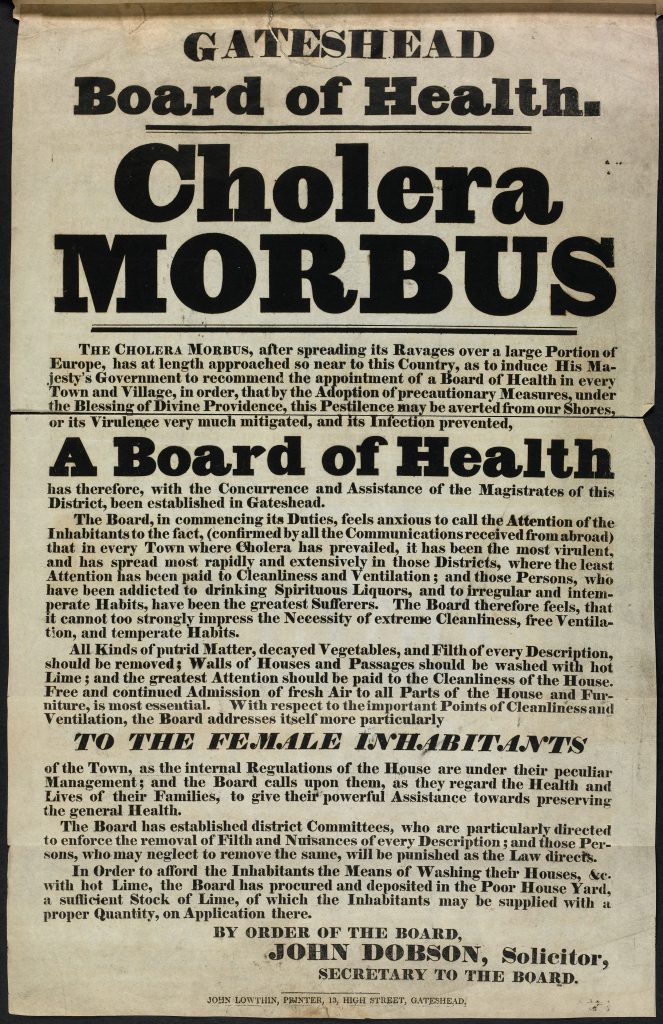
The understanding that the widespread and sudden outbreak was closely associated with housing conditions and filth led public health reformers to advocate that active measures, such as cleaning, drainage and ventilation, would improve London’s working people health. Thus, structural changes were enacted with a series of laws, such as the Cholera Morbus Prevention Act, the Nuisances Removal and Diseases Prevention Act and The Sewerage and Drainage of Liverpool Act etc. New governmental bodies were set up such as the Metropolitan Commission of Sewers and the Metropolitan Board of Works after the Metropolis Management Act was passed.
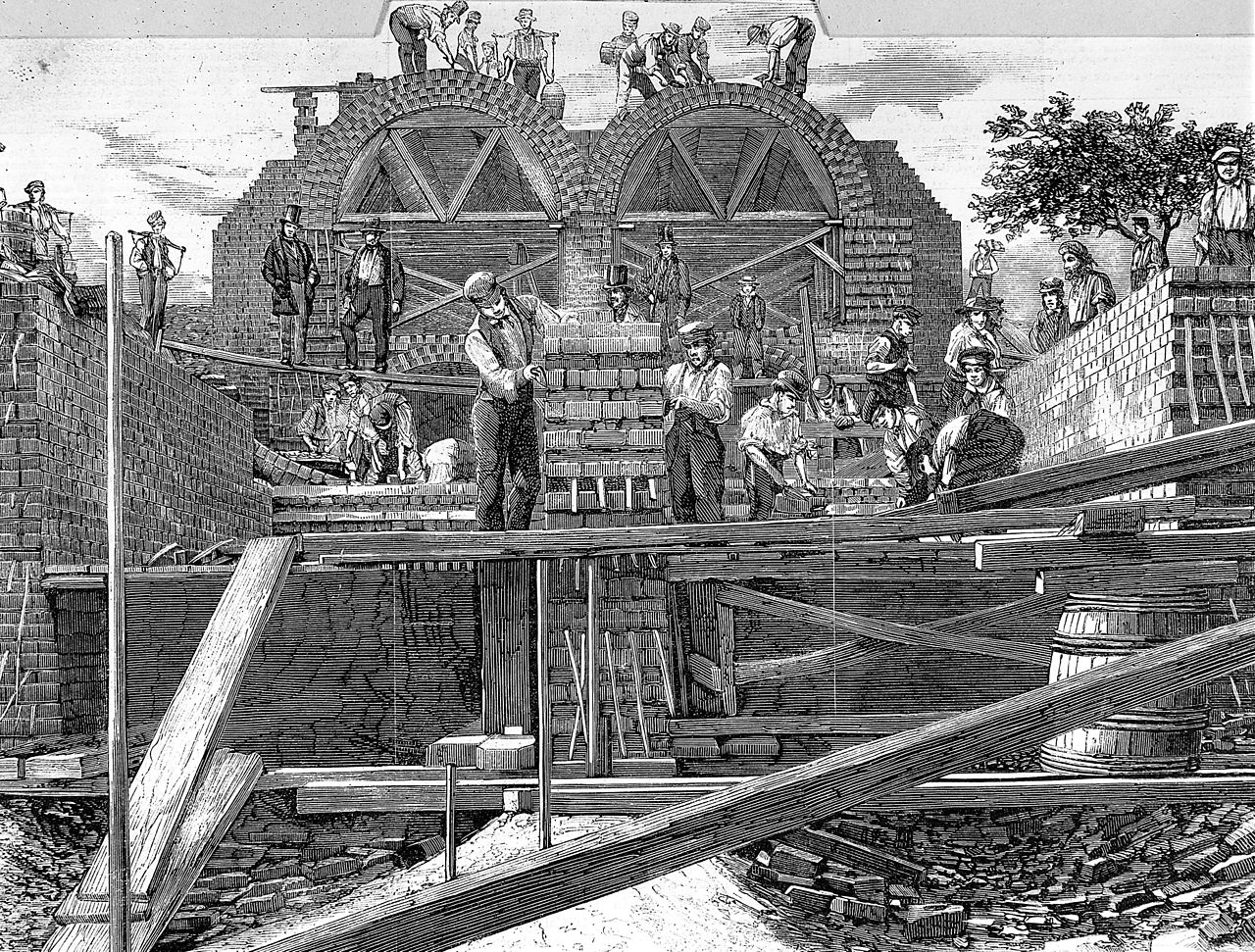
Importantly, parliament authorized a new sewer network for London, in what became one of the century’s great engineering projects. Even the river Thames was refitted to better handle London’s sewage. Thus, by accepting scientific findings and acting accordingly with city-wide structural change could cholera be prevented “from becoming a common nuisance in the social organization.”
QUESTION: GLOBALSTRUCTURAL CHANGES?
The open question is whether analogs of the structural changes to London that stemmed cholera’s tide will happen with Covid. Will today’s London elite…the Developed world… take actions that benefit the entire of today’s London … the world?
If we focus on providing vaccines to the unvaccinated, it’s evident what doing nothing will result in. Global health researchers caution that this strategy will promote conditions that prolong the pandemic. The continued spread of Covid among the majority of humanity remaining unvaccinated are precisely the conditions needed for the rise of dangerous variants that will eventually escape vaccine or infection related immune responses. This could set up conditions where both the Developed and Developing world will always be at risk from new variants. More infectious and virulent Covid variants could likely disrupt the revival of the global economy with estimates of US $4.5 trillion being eliminated from the global gross domestic product by 2025.
ANSWER: PROTECT YOURSELF BY PROTECTING EVERYONE
We can learn from our Victorian predecessors and reason as they did. Just as London’s wealthy registered that their protection depended on the protection of all their city’s people, so Developed world must learn that they can only protect their health if they protect the health of all the world’s people.
A first step of paramount importance is vaccinating everyone who have received no doses. That means that booster shots should wait till sufficient numbers of people are vaccinated world-wide to inhibit the rise of more dangerous variants. In fact, the benefits of boosters to people already vaccinated is minimal compared to the benefits from inoculating the unvaccinated. This way, we can get way more vaccination bang for the buck!
The vaccination rate in the Developing world needs to increase 19-fold to immunize 40% of the unvaccinated by 2022. The alternative, according to the West coast NGO KFF, is maintain the current vaccination rates thereby providing significant Covid protection by early 2023.
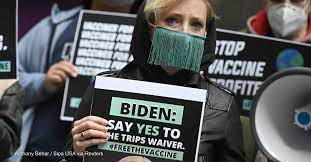
Thus, the first step in analogous structural changes in the world’s public health systems is Universal Covid Vaccination. Booster vaccinations can be a sensible longer-term measure for global health, but only when Covid vaccine shortages end or the current vaccines are no longer effective against new variants. A more significant structural change would be to reform global Intellectual Property Rights to allow those countries in the Developing world to manufacture their own vaccines.
Further structural changes could include the prevention and treatment of the many other infectious diseases afflicting millions in the Developing world. While Covid caused 2 million deaths in 2020, malaria kills 3 million people per year for decades.
Just as the experience of London and other European cities had with cholera demonstrated the benefits of public health reform, so can those experiences inform our current global public health crisis. The Victorian lesson for Covid is that our health depends on the world’s health.
E. Ashworth Underwood, “The History of Cholera in Great Britain”, 1947, Section of Epidemiology and State Medicine, Proceedings of the Royal Society of Medicine, vol 165, p1
The Cholera Years, the United States in 1832, 1849 and 1866 Charles Rosenberg 1962